
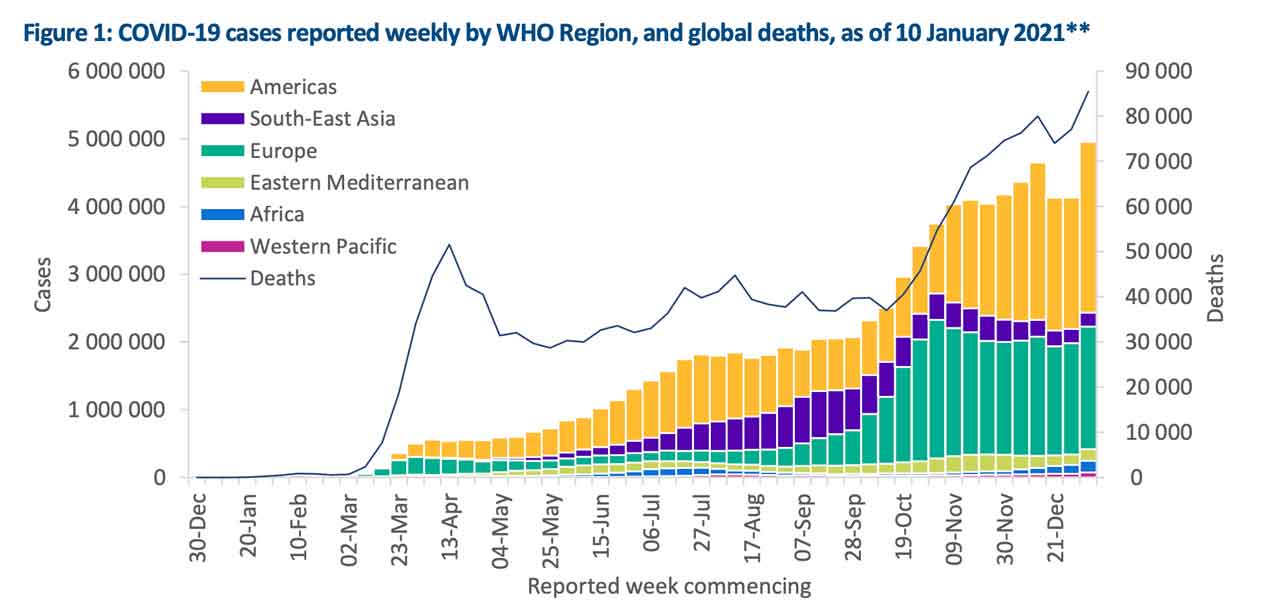
The World Health Organization says “Following two weeks of low reporting, likely due to the year-end holiday period, the overall upward trend seen in earlier weeks has resumed, with just under 5 million new cases reported last week globally.”
The global trends have changed since then.
WHO says, “The number of new deaths has also shown a similar trend, with over 85 000 reported last week, an 11% increase. All regions apart from South-East Asia showed an increase in new cases, with the Western Pacific, Africa and the Americas reporting increases of over 30%.
The Region of the Americas accounted for 51% of all new cases and 45% of all new deaths globally in the past week.
The European Region had a lower increase in new cases (10%), however still accounts for over a third of new cases globally.

In South-East Asia, the decline in new cases and new deaths seen since the end of November 2020 continues. Although the Eastern Mediterranean Region is showing an 11% increase in new cases, new deaths have fallen by 9%, continuing a downward trend since a peak in mid-November.
The African Region reported 175 000 new cases and 4300 new deaths, an increase of over 30% in new cases and new deaths, far exceeding previous peaks in July 2020. The Western Pacific also reported an increase of more than 30% in new cases, while the number of new deaths also rose by 14%.
In the past week, the five countries reporting the highest number of cases were the United States of America (with 1,786,773 cases, a 35% increase), the United Kingdom of Great Britain and Northern Ireland (417,620 cases, a 22% increase), Brazil (313,130 cases, a 24% increase), the Russian Federation (165,167 cases, continuing last week’s decrease with an 12% decrease) and Germany (142,861 cases, reversing last week’s decrease with a 15% increase).
Additional Region-specific information can be found below: African Region, Region of the Americas, Eastern Mediterranean Region, European Region, South-East Asia Region, and Western Pacific Region.
Please note: New cases and deaths will be reported per 100 000 population instead of per 1 million population, starting from this report.
SARS-CoV-2 Variants of concern
Since the start of the COVID-19 pandemic, WHO has received several reports of public health events associated with variants of SARS-CoV-2. When considered to potentially have different epidemiological, immunological or pathogenic properties, variants are reported to WHO and raised for further investigation by national authorities.
Further background on variants of concern (VOC) is available in Disease Outbreak News and the Weekly Epidemiological Update published 5 January. In collaboration with local authorities, institutions and researchers, WHO routinely assesses if variants of SARS-CoV-2 result in changes in transmissibility, clinical presentation and severity, or if they may impact on countermeasures, including diagnostics, therapeutics and vaccines. While investigations are ongoing, in the following update, we highlight the geographical extent of two variants – VOC 202012/01 (initially identified in the United Kingdom) and 501Y.V2 (initially identified in South Africa) – reported by countries, territories and areas as of 12 January 2021, as well as highlight recent reports of other new variants of potential concern.
Since first detected on 14 December 2020, VOC 202012/01 has been detected in 50 countries, territories and areas across five of the six WHO regions to date (Figure 3). In England, the variant has been detected in all regions and almost all local authorities. Here, investigations are using a proxy S gene target failure (SGTF) to indicate carriage of the VOC, as only a small proportion of these variants is detected using whole genome sequencing, which lags approximately two weeks behind the initial test date. Results show that the age and sex distribution of VOC 202012/01, as determined by SGTF, is similar that of other variants in circulation over the same period. Analyses using contact tracing data showed higher transmissibility (secondary attack rates) where the index case has the variant strain, from around 11% to 15% of named contacts.
Since first reported on 18 December 2020, variant 501Y.V2 has been detected in 20 countries, territories and areas across four of the six WHO regions (Figure 4). From preliminary and ongoing investigations in South Africa, it is possible that the 501Y.V2 variant is more transmissible than variants circulating in South Africa previously. Moreover, while this new variant does not appear to cause more severe illness, the observed rapid increases in case numbers has placed health systems under pressure.
On 9 January, Japan notified WHO of a new SARS-CoV-2 variant within lineage B.1.1.28 (initially reported as B.1.1.248) detected in four travelers arriving from Brazil. This variant has 12 mutations to the spike protein, including three mutations of concern in common with VOC 202012/01 and 501Y.V2, i.e.: K417N/T, E484K and N501Y, which may impact transmissibility and host immune response. Researchers in Brazil have additionally reported the emergence of a similar variant also with a E484K mutation, which has likely evolved independently of the variant detected among Japanese travelers. The extent and public health significance of these new variants require further investigation.
It is well known that viruses constantly change through mutation, and so the emergence of new variants is an expected occurrence. Many mutations have no impact on the virus itself while some could be detrimental to the virus and few may result in an advantage to the virus. These variants of concern identified in different countries highlight the importance of increasing diagnostic capacity and systematic sequencing of SARS-CoV-2 where capacity allows, as well as the timely sharing of sequence data internationally.
Systematic sequencing should be considered for a subset of incoming travellers, as well as community-based samples to ascertain the existence and extent of local transmission. The geographical extent of both VOC 202012/01 and 501Y.V2 reported above is likely underestimated given a bias toward countries/territories/areas detecting the variants with sequencing capacity, and where surveillance systems have been adapted to detect these new variants. Irrespective of sequencing capacity in countries, surveillance through established systems and regular epidemiology analyses should continue to inform adjustments to public health and social measures. Research is ongoing to determine the impact of new variants on transmission, disease severity as well as any potential impacts on vaccines, therapeutics and diagnostics. These efforts will require coordination of research between WHO, partners and groups of international scientists (WHO Virus Evolution Working Group).