
-
Globally, one in three people drink alcohol (equivalent to 2.4 billion people), and 2.2% of women and 6.8% of men die from alcohol-related health problems each year.
-
Alcohol use was ranked as the seventh leading risk factor for premature death and disability worldwide in 2016, and was the leading cause for people aged 15-49 years old. In this age group, it is associated with tuberculosis, road injuries, and self-harm.
-
For people aged 50 years and older, cancers were a leading cause of alcohol-related death, constituting 27.1% of deaths in women and 18.9% of deaths in men.
-
The authors suggest there is no safe level of alcohol as beneficial effects against ischemic heart disease are outweighed by the adverse effects on other areas of health, particularly cancers.
THUNDER BAY – HEALTH – The impact of alcohol can be seen across Northern Ontario. Like many northern regions across the globe, the use of alcohol is greater in northern climates. The impact of alcohol on health, on social services, families and the lives of millions is massive.
A new study states that alcohol is a leading risk factor for death and disease worldwide, and is associated with nearly one in 10 deaths in people aged 15-49 years old. This information comes according to a Global Burden of Disease study published in The Lancet that estimates levels of alcohol use and health effects in 195 countries between 1990 to 2016.
Based on their analysis, the authors suggest that there is no safe level of alcohol as any health benefits of alcohol are outweighed by its adverse effects on other aspects of health, particularly cancers.
They estimate that, for one year, in people aged 15-95 years, drinking one alcoholic drink a day [1] increases the risk of developing one of the 23 alcohol-related health problems [2] by 0.5%, compared with not drinking at all (from 914 people in 100,000 for one year for non-drinkers aged 15-95 years, to 918 in 100,000 people a year for 15-95 year olds who consume one alcoholic drink a day) [3].
Alcohol has a complex association with health, affecting it in multiple ways. Regular consumption has adverse effects on organs and tissues, acute intoxication can lead to injuries or poisoning, and alcohol dependence may lead to frequent intoxication, self-harm or violence. Some previous research has suggested that low levels of consumption can have a protective effect against heart disease and diabetes.
“Previous studies have found a protective effect of alcohol on some conditions, but we found that the combined health risks associated with alcohol increase with any amount of alcohol. In particular, the strong association between alcohol consumption and the risk of cancer, injuries, and infectious diseases offset the protective effects for ischaemic heart disease in women in our study. Although the health risks associated with alcohol starts off being small with one drink a day, they then rise rapidly as people drink more,” says lead author Dr Max Griswold, Institute for Health Metrics and Evaluation, University of Washington, USA. “Policies focussing on reducing alcohol consumption to the lowest levels will be important to improve health. The widely held view of the health benefits of alcohol needs revising, particularly as improved methods and analyses continue to shed light on how much alcohol contributes to global death and disability.” [4]
Robust estimates of alcohol consumption and related risks
The study used data from 694 studies to estimate how common drinking alcohol is worldwide and used 592 studies including 28 million people worldwide to study the health risks associated with alcohol [2] between 1990 to 2016 in 195 countries. In the study, a standard alcoholic drink is defined as 10g alcohol [1].
Previous studies looking at these risks rely on self-reported surveys and alcohol sales data to estimate consumption levels. These have limitations, including that non-drinkers may avoid alcohol as they have health issues, they do not take into account types of alcohol that are not purchased (such as illicit trade and home brewing), and most studies assume that not drinking minimises risk but do not study the association to confirm this.
The new study provides more robust estimates of alcohol consumption by combining alcohol sales data with the prevalence of alcohol drinking and abstinence, self-reported data on the amount of alcohol drank, tourism data to estimate the number of alcohol-drinking visitors to an area, and estimating levels of illicit trade and home brewing.
It also includes a new, more robust systematic review and meta-analysis of alcohol consumption and the associated health problems, which used specific controls to reduce confounding factors. It also used a new statistical method to more accurately estimate the risks related to drinking between 0-15 standard drinks each day. The authors used this to estimate the amount of alcohol exposure that would minimise an individual’s risk of alcohol-related health problems.
Global alcohol consumption
Globally, one in three people (32.5%) drink alcohol – equivalent to 2.4 billion people – including 25% of women (0.9 billion women) and 39% of men (1.5 billion men). On average, each day women consumed 0.73 alcoholic drinks, and men drank 1.7 drinks.
Drinking patterns varied globally [5], the highest number of current alcohol drinkers was in Denmark (95.3% of women, and 97.1% of men) while the lowest were in Pakistan for men (0.8%) and Bangladesh for women (0.3%). Men in Romania and women in Ukraine drank the most (8.2 and 4.2 drinks a day respectively), whereas men in Pakistan and women in Iran drank the least (0.0007 and 0.0003 drinks a day respectively).
Risks associated with alcohol
Globally, drinking alcohol was the seventh leading risk factor for premature death and disease in 2016, accounting for 2.2% of deaths in women and 6.8% of deaths in men. However, in people aged 15-49 years old, alcohol was the leading risk factor in 2016, with 3.8% of deaths in women and 12.2% of deaths in men attributable to alcohol.
The main causes of alcohol-related deaths in this age group were tuberculosis (1.4% of deaths), road injuries (1.2%), and self-harm (1.1%). For people aged 50 years and older, cancers were a leading cause of alcohol-related death, constituting 27.1% of deaths in women and 18.9% of deaths in men.
The health problems associated with alcohol at age 50 or older varied depending on region. In high-income countries, cancers were the most common alcohol-related premature death and disease, while in low-income countries tuberculosis was the leading cause, followed by cirrhosis and chronic liver diseases. In middle- and high-to-middle income countries stroke was the main alcohol-related burden.
The authors found that there was only a protective effect between alcohol and ischemic heart disease, and there were possible protective effects for diabetes and ischemic stroke but these were not statistically significant. The risk of developing all other health problems increased with the number of alcoholic drinks consumed each day.
Combining these findings, the protective effect of alcohol was offset by the risks and overall the health risks associated with alcohol rose in line with the amount consumed each day. Therefore, the authors conclude that there is no safe level of alcohol.
Specifically, comparing no drinks with one drink a day the risk of developing one of the 23 alcohol-related health problems was 0.5% higher – meaning 914 in 100,000 15-95 year olds would develop a condition in one year if they did not drink, but 918 people in 100,000 who drank one alcoholic drink a day would develop an alcohol-related health problem in a year.
This increased to 7% in people who drank two drinks a day (for one year, 977 people in 100,000 who drank two alcoholic drinks a day would develop an alcohol-related health problem) and 37% in people who drank five drinks every day (for one year, 1252 people in 100,000 who drank five alcoholic drinks a day would develop an alcohol-related health problem) [3].
Professor Emmanuela Gakidou, Institute for Health Metrics and Evaluation, University of Washington, USA, says: “Alcohol poses dire ramifications for future population health in the absence of policy action today. Our results indicate that alcohol use and its harmful effects on health could become a growing challenge as countries become more developed, and enacting or maintaining strong alcohol control policies will be vital.”
“Worldwide we need to revisit alcohol control policies and health programmes, and to consider recommendations for abstaining from alcohol. These include excise taxes on alcohol, controlling the physical availability of alcohol and the hours of sale, and controlling alcohol advertising. Any of these policy actions would contribute to reductions in population-level consumption, a vital step toward decreasing the health loss associated with alcohol use.” [4]
The authors note some limitations, including that it is difficult to estimate illicit alcohol production and unrecorded consumption so their results may not fully capture this. The study also does not include drinking data for people under the age of 15 years, and does not include links to health problems such as dementia and psoriasis where evidence suggests alcohol could be a risk factor. The authors say that this may mean their study underestimates the number of people drinking alcohol and the risks associated.
In addition, there was little robust data on interpersonal violence due to alcohol, and the data for road accidents due to alcohol that cause harm to others were based on USA data only. While patterns are unlikely to vary around the world, this needs to be confirmed.
Because more in-depth information is not available, the study assumes that drinking patterns are the same across the year, but previous research suggests that changing drinking patterns, such as binge-drinking, could be linked to different levels of risk.
Writing in a linked Comment, Dr Robyn Burton, King’s College London, UK, calls the study the most comprehensive estimate of the global burden of alcohol use to date. She says: “The conclusions of the study are clear and unambiguous: alcohol is a colossal global health issue and small reductions in health-related harms at low levels of alcohol intake are outweighed by the increased risk of other health-related harms, including cancer. There is strong support here for the guideline published by the Chief Medical Officer of the UK who found that there is “no safe level of alcohol consumption”. The findings have further ramifications for public health policy, and suggest that policies that operate by decreasing population-level consumption should be prioritised… These diseases of unhealthy behaviours, facilitated by unhealthy environments and fuelled by commercial interests putting shareholder value ahead of the tragic human consequences, are the dominant health issue of the 21st century. The solutions are straightforward: increasing taxation creates income for hard-pressed health ministries, and reducing the exposure of children to alcohol marketing has no downsides.”
Peer-reviewed / Observational study / People
This study was funded by the Bill & Melinda Gates Foundation. It was conducted by researchers from the GBD 2016 Alcohol Collaborators (full list at the end of the Article).
[1] One standard drink is defined as 10 grams of pure alcohol. Examples include:
- A small glass of red wine (100ml or 3.4 fluid ounces) at 13% alcohol by volume;
- A can or bottle of beer (375 ml or 12 fluid ounces) at 3.5% alcohol by volume; or
- A shot of whiskey or other spirits (30 ml or 1.0 fluid ounces) at 40% alcohol by volume.
[2] These health issues include:
- Cardiovascular diseases: atrial fibrillation and flutter, hemorrhagic stroke, ischemic stroke, hypertensive heart disease, ischemic heart disease, and alcohol cardiomyopathy;
- Cancers: breast, colorectal, esophageal, larynx, lip and oral cavity, liver, and nasal and mouth cavities;
- Other non-communicable diseases: cirrhosis of the liver due to alcohol use, diabetes, epilepsy, pancreatitis, and alcohol use disorders;
- Communicable diseases: lower respiratory infections, and tuberculosis;
- Intentional injuries: interpersonal violence, and self-harm;
- Unintentional injuries: exposure to mechanical forces, poisonings, fire, heat, and hot substances, drowning, and other unintentional injuries; and
- Transportation-related injuries.
[3] The relative risk associated with 0-15 alcoholic drinks is available in Figure 5 of the paper. The absolute risks used to calculate this are provided by the authors.
[4] Quote direct from author and cannot be found in the text of the Article.
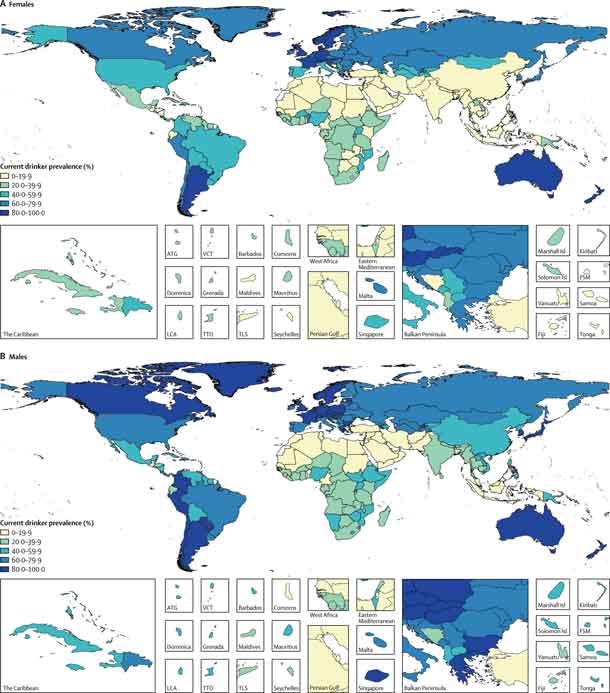
[5] Prevalence of current drinkers in 2016:
Males
Highest prevalence:
- Denmark: 97.1
- Norway: 94.3
- Argentina: 94.3
- Germany: 94.3
- Poland: 93.8
- France: 93.1
- South Korea: 91.3
- Switzerland: 91.2
- Greece: 90.8
- Iceland: 90.3
Lowest prevalence:
- Pakistan: 0.9
- Bangladesh: 1.0
- Egypt: 1.1
- Mali: 2.5
- Morocco: 3.0
- Senegal: 3.2
- Mauritania: 3.2
- Syria: 5.0
- Indonesia: 7.2
- Palestine: 7.9
Females
Highest prevalence:
- Denmark: 95.3
- Norway: 91.4
- Germany: 90.0
- Argentina: 89.9
- New Zealand: 88.5
- Switzerland: 88.4
- Slovakia: 87.2
- France: 86.9
- Sweden: 86.1
- Iceland: 84.8
Lowest prevalence:
- Bangladesh: 0.3
- Morocco: 1.1
- Pakistan: 1.5
- Egypt: 1.5
- Nepal: 1.5
- Syria: 1.6
- Bhutan: 1.9
- Myanmar: 2.3
- Tunisia: 2.3
- Senegal: 2.6
Average number of daily drinks in 2016:
Males
Greatest number of drinks:
- Romania: 8.2
- Portugal: 7.3
- Luxembourg: 7.3
- Lithuania: 7.0
- Ukraine: 7.0
- Bosnia and Herzegovina: 6.5
- Belarus: 6.0
- Estonia: 6.0
- Spain: 5.8
- Hungary: 5.5
Lowest numbest of drinks:
- Pakistan: 0.0008
- Iran: 0.004
- Kuwait: 0.02
- Comoros: 0.02
- Libya: 0.02
- Bangladesh: 0.03
- Palestine: 0.04
- Mauritania: 0.05
- Yemen: 0.05
- Saudi Arabia: 0.05
Females
Highest number of drinks:
- Ukraine: 4.2
- Andorra: 3.4
- Luxembourg: 3.4
- Belarus: 3.4
- Sweden: 3.2
- Denmark: 3.2
- Ireland: 3.1
- United Kingdom: 3.0
- Germany: 2.9
- Switzerland: 2.8
Lowest number of drinks:
- Iran: 0.0003
- Kuwait: 0.01
- Mauritania: 0.02
- Libya: 0.02
- Pakistan: 0.03
- Timor-Leste: 0.04
- Palestine: 0.04
- Yemen: 0.04
- Tunisia: 0.04
- Syria: 0.05





